


Axial S-1 Club - Cullinan Oncology
Surveying great inventors and businesses
Axial partners with great founders and inventors. We invest in early-stage life sciences companies such as Appia Bio, Seranova Bio, Delix Therapeutics, Simcha Therapeutics, among others often when they are no more than an idea. We are fanatical about helping the rare inventor who is compelled to build their own enduring business. If you or someone you know has a great idea or company in life sciences, Axial would be excited to get to know you and possibly invest in your vision and company . We are excited to be in business with you - email us at info@axialvc.com

Cullinan Oncology was founded in 2016 to build a hub-and-spoke business model for oncology drug development. Their recent S-1 highlights the company’s focus on capital efficiency and building a large and diversified pipeline of drug candidates. Technically, Cullinan requires one of two features before advanced a candidate into the clinic:
Drug candidate generates a strong immune response
Drug candidate can inhibit a target as a monotherapy
The company has 1 drug candidate in phase 1/2 development along with 6 in pre-clinical development. Cullinan’s goal is to bring at least one new drug into the clinic each year. Their lead candidate, CLN-081, is a small molecule inhibitor of epidermal growth factor receptor (EGFR) with an exon 20 insertion to treat patients with non-small cell lung cancer (NSCLC).
Highlights
Cullinan’s lead asset, CLN-081, targets EGFRex20ins, which is found in around 10% of all EGFR mutations in NSCLC. Overall, EGFR mutations are found in around 20% of all NSCLC patients. This leads to an incidence rate for NSCLC patients with EGFRex20ins at 2K-5K in the US and ~2K in Europe.
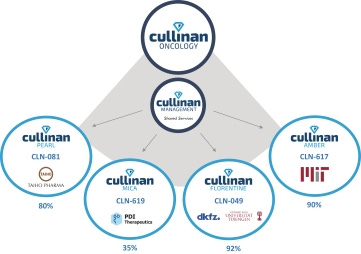
The company uses a hub-and-spoke business model: the hub is Cullinan Oncology, LLC and the operating company, Cullinan Management, Inc. The spokes are a separate company with its own pipeline of drug candidates. The hub provides the spokes capital and operational resources to create synergies that reduce cost.
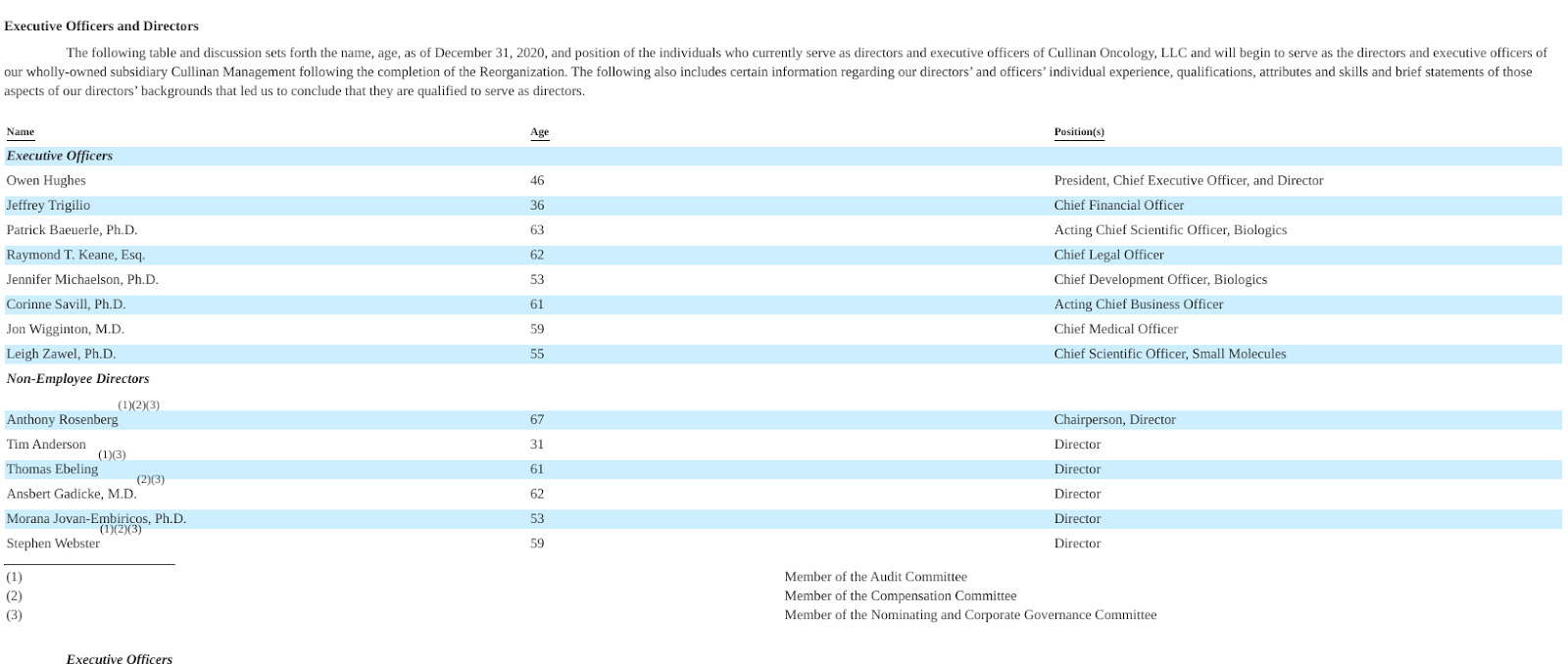
Team
Cullinan’s CEO since 2017 is Owen Hughes. He was the Chief Business Officer and Head of Corporate Development at Intarcia Therapeutics and worked at Brookside Capital, a hedge fund owned by Bain Capital. Cullinan’s CSO is Patrick Baeuerle who co-founded the company - previously, he was a VP of Research at Amgen, CSO at Micromet, and head of small molecule drug discovery at Tularik. With MPM Capital, Baeuerle also co-founded companies like Harpoon Therapeutics, Maverick Therapeutics, and TCR² Therapeutics.
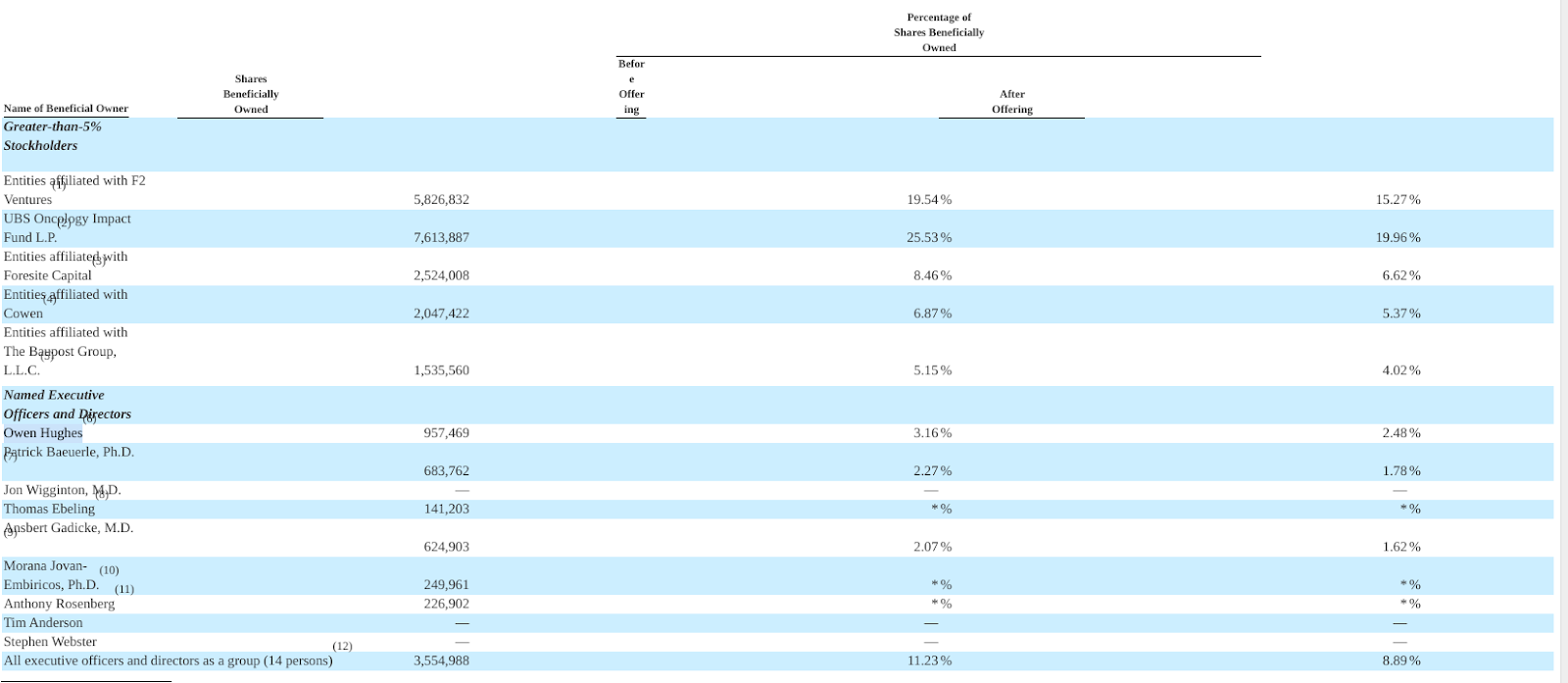
Investors
The company’s main investors are Foresite Capital, F2 Ventures, and the UBS Oncology Impact Fund (managed by MPM Capital). Cullinan’s Series was led by F2 and UBS in 2017, and the company ultimately raised $277M (spending $60M) across private financing rounds.
Technology
Cullinan has 5 major assets in development (with descriptions from the S-1 below):
CLN-081 - NSCLC
CLN-049 - AML
CLN-619 - pan-cancer
CLN-617 - pan-cancer
CLN-978 - B-cell ALL
“CLN-081 is an orally available small molecule designed as a next generation, irreversible EGFR inhibitor in development for the treatment of a genetically defined subset of patients with NSCLC. CLN-081 is being developed by our partially-owned subsidiary Cullinan Pearl, and is currently in a Phase 1/2a dose escalation and expansion trial evaluating oral, twice-daily, or BID, administration of various doses in patients with NSCLC harboring EGFRex20ins mutations that have had at least one prior treatment with platinum based chemotherapy or another approved standard therapy. We licensed worldwide rights, excluding Japan, to CLN-081 from Taiho Pharma in 2018, and we recently sublicensed such rights to Zai Lab (Shanghai) Co., Ltd. in Greater China in exchange for an upfront fee, milestones, and royalties. For additional information, see “License Agreements—Zai Lab License Agreement.” In September 2020, at the European Society for Medical Oncology virtual congress, we disclosed preliminary results based on the first 22 patients dosed in this ongoing trial. As of September 1, 2020, amongst 17 evaluable patients across all dose cohorts, we observed a best overall response of partial response in six patients and stable disease in 11 patients. The partial responses included two confirmed and four unconfirmed partial responses, three of whom had not yet reached a confirmatory scan and one who progressed prior to a confirmatory scan. As of the September 1, 2020 data cut-off, no dose limiting toxicities, or DLTs, or Grade 3 treatment-related adverse events, or TRAEs, had been reported. As of the November 10, 2020 data cut-off, amongst 25 evaluable patients across all dose cohorts, we observed a best overall response of partial response in 10 patients, stable disease in 14 patients, and disease progression in one patient. The partial responses included six confirmed and four unconfirmed partial responses, two of whom had not yet reached a confirmatory scan. Regarding the two remaining patients with unconfirmed partial responses, one experienced progressive disease due to a new brain lesion and one died before their second scan after experiencing aspirational pneumonia that was deemed unrelated to study drug by the investigator. As of the November 10, 2020 data cut-off, we observed one DLT, which was Grade 3 diarrhea TRAE in the 150mg BID dosing cohort, our highest dose evaluated to date, and one other Grade 3 TRAE, which was anemia. We observed no Grade 2 diarrhea TRAEs in the 30, 45, 65, or 100mg BID dose cohorts. We observed one Grade 2 diarrhea TRAE in the 150mg BID dose cohort. As of the November 10, 2020 data cutoff, we observed eight Grade 2 skin rash TRAEs across all dose cohorts. Although these results are preliminary and based on a small number of patients with limited follow-up, we believe that the preclinical and early clinical data as of the data cut-off collectively support the potential of CLN-081 to be a clinically active molecule with a favorable product profile. Given the trial was designed as a dose escalation and expansion study, we anticipate observing additional TRAEs as we enroll more patients and follow them over longer duration periods at higher dose levels. We intend to provide a clinical update in the first half of 2021.
CLN-049 is a humanized bispecific antibody that we are developing at our partially-owned subsidiary Cullinan Florentine for the treatment of AML. CLN-049 is designed to simultaneously bind to FLT3 on target leukemic cells and to CD3 on T cells, triggering the T cells to kill the targeted cancer cells via their intrinsic cytolytic mechanisms. FLT3 is expressed frequently on AML cells and leukemic blasts but minimally on healthy blood cells, unlike other tumor surface antigens identified in AML, such as CD33 and CD123. We believe that the expression of FLT3 on the surface of leukemic blasts in most AML patients and its role as a known oncogenic driver make it an attractive therapeutic target for a T cell engager approach. Furthermore, by targeting the extracellular domain of FLT3, we believe CLN-049 has the potential to address a broader patient population than existing small molecule FLT3 kinase inhibitors acting within the intracellular domain, but are limited to a subset of approximately 25% of AML patients with certain mutations. We have observed that CLN-049 led to potent FLT3-dependent killing of leukemic cells in vitro at a wide range of FLT3 expression levels on AML cells. In preclinical studies, treatment with CLN-049, even at low doses, led to survival benefit in an AML xenograft model and complete elimination of leukemic blasts in various mouse models implanted with primary patient leukemic cells or AML cell lines. We have completed IND-enabling pharmacology, pharmacokinetic, and safety studies, and we expect to submit our IND for CLN-049 in the first quarter of 2021.
CLN-619, which is being developed by our partially-owned subsidiary Cullinan MICA, is a MICA/B-targeted, humanized IgG1 monoclonal antibody that we are initially developing for the treatment of patients with advanced solid tumors. CLN-619 was designed to promote an antitumor response through multiple mechanisms of action, including engagement of NK and T cells for enhanced lysis of cancer cells. The MICA/B receptor, NKG2D, is expressed in both innate and adaptive effector cell populations. Although several companies have disclosed preclinical programs targeting MICA/B, we are unaware of any clinical-stage programs in development. In preclinical studies, CLN-619 demonstrated antitumor activity as a single agent in multiple in vivo models. We believe CLN-619 has the potential to become a novel backbone agent for immuno-oncology therapy given the broad expression of MICA/B across tumor types and the biologic rationale for combining CLN-619 with other agents. We have completed IND-enabling pharmacology and toxicology studies and are completing good manufacturing practice, or GMP, process work to support an IND submission in the first half of 2021.
We are also developing CLN-617, a fusion protein uniquely combining, in a single agent, two antitumor cytokines, IL-2 and IL-12, with a collagen-binding domain for the treatment of solid tumors. This collagen-binding domain is designed to retain the cytokines in the tumor microenvironment following intratumoral administration, with the goal of minimizing systemic dissemination and associated toxicities of cytokines while prolonging their immunostimulatory antitumor activity. For nearly five decades, clinical researchers have characterized the powerful role cytokines play in stimulating an immune response to cancer. However, despite numerous advancements in protein engineering, delivery and targeting mechanisms, the short serum half-life and severe toxicities associated with systemic cytokine administration have hindered their clinical development and commercial uptake. We believe that CLN-617, by utilizing a collagen-binding domain, has the potential to address these shortcomings and is the only anti-cancer therapeutic candidate in development that we are aware of that combines IL-2 and IL-12. In preclinical studies, murine surrogates of CLN-617 demonstrated robust single agent antitumor activity in both injected and non-injected contralateral tumors without inducing systemic toxicity, as measured by reduction in body weight. Based on these results, we believe CLN-617 may be capable of generating a systemic immune response that can mediate tumor regression, even in non-injected distal tumors. Given the broad expression of collagens across multiple tumor types and the well-validated antitumor activity of cytokine-based therapies, CLN-617 may have utility across many different types of solid tumors. CLN-617 is being developed by our partially-owned subsidiary Cullinan Amber, and we expect to submit an IND for CLN-617 in 2022. We refer to the collagen-binding technology used in CLN-617 as AMBER, which we believe represents a novel platform with the potential to broaden the therapeutic window of cytokines and other immunostimulatory agents by potentially reducing systemic toxicity.
CLN-978 is a half-life extended, humanized, single-chain T cell engaging antibody construct designed to simultaneously engage CD19 on target cancer cells and CD3 on T cells, triggering redirected T cells to lyse the target cancer cells. In addition to CD19 and CD3 binding domains, CLN-978 has a human serum albumin binding antibody domain, which is designed to prolong its serum half-life. We believe that by potentially extending the serum half-life of CLN-978, we can address limitations related to the dosing regimen of blinatumomab, the only CD19-targeting bispecific T cell engager approved for the treatment of relapsed or refractory B-cell acute lymphoblastic leukemia, or ALL, and potentially offer unique advantages and broader access for patients. CLN-978, referred to as NexGem, mediated highly potent CD19-dependent target cell lysis in vitro at various CD19 target expression levels. In preclinical in vivo studies, treatment with NexGem, at extremely low doses and with infrequent dosing, led to inhibition of tumor growth and tumor regression in a human CD3e transgenic lymphoma mouse model. CLN-978 is held in our wholly-owned subsidiary Cullinan Management, Inc. We intend to initially evaluate CLN-978 as a novel treatment for B-cell ALL, and expect to submit our IND for CLN-978 in 2022.”

Market
Cullinan’s lead asset, CLN-081, targets EGFRex20ins, which is found in around 10% of all EGFR mutations in NSCLC. Overall, EGFR mutations are found in around 20% of all NSCLC patients. This leads to an incidence rate for NSCLC patients with EGFRex20ins at 2K-5K in the US and ~2K in Europe. Given that CLN-081 is a first-in-class medicine, the entire patient population is addressable. The company’s pipeline expands to indications with larger patient populations like AML and ALL; however, the focus on a small disease group is important to increase the odds of success and validate Cullinan’s approach.
Business model
The company uses a hub-and-spoke business model: the hub is Cullinan Oncology, LLC and the operating company, Cullinan Management, Inc. The spokes are a separate company with its own pipeline of drug candidates. The hub provides the spokes capital and operational resources to create synergies that reduce cost. Using shared resources ought to maintain a controlled cost structure as Cullinan’s pipeline grows.
For example internal programs in early stages can use the hub’s services in discovery and optimization before clinical work. Moreover, licensing agreements and collaborations can be put into separate spokes. Importantly, each spoke has a distinct cap table, which gives Cullinan to incentivize management with equity and raise capital at the parent and subsidiary levels.
Valuation
Cullinan’s valuation is driven by both the success of its pipeline as well as its cost structure over time:
The company is working to build a diversified and hopefully uncorrelated, by modality, stage and MoA, oncology pipeline
Expand Cullinan’s research collaborations and partnerships
Bringing CLN-081 to a pivotal study
Expand their pipeline of immuno-oncology drugs
Have an IND-enabling study each year

Mention highlights in the S-1
Patent: 318
FDA: 290
Research: 246
Cancer: 117
NSCLC: 43
Licensing: 44
Hub-and-spoke: 22
Cytokine: 20