Axial Discovery - Targeting cardiac fibrosis with engineered T-cells
Call for talented individuals and teams
Axial: https://linktr.ee/axialxyz
Axial partners with great founders and inventors. We invest in early-stage life sciences companies such as Appia Bio, Seranova Bio, Delix Therapeutics, Simcha Therapeutics, among others often when they are no more than an idea. We are fanatical about helping the rare inventor who is compelled to build their own enduring business. If you or someone you know has a great idea or company in life sciences, Axial would be excited to get to know you and possibly invest in your vision and company . We are excited to be in business with you - email us at info@axialvc.com

Targeting cardiac fibrosis with engineered T-cells
A landmark Nature paper in 2019 first demonstrated the use of CAR-T cell therapies against FAP, a fibrosis–related target. The work came out of the Jonathan Epstein lab at Penn, and a follow-up study published in early 2022 built on the past work to establish in vivo activity of CAR-T cells after delivery (IV, CD5-targeted LNPs) of an anti-FAP chimeric antigen receptor (CAR) with mRNA. Capstan Therapeutics was publicly launched later in the year to commercialize this technology and develop in vivo cell therapies. The research gives a path for the development of cell therapies for fibrosis and more companies like Capstan will sprout up. However, the research is more interesting for unveiling a compelling mechanism to treat fibrosis regardless if it’s a cell therapy, bispecific, or something else.
Existing therapies limit fibrosis but cannot reverse or remodel it. For cardiovascular disease, you still have things like beta blockers being used for symptomatic support. New treatments to go after the underlying cause are emerging. For example, MyoKardia pioneered a precision medicine approach to develop mavacamten for obstructive HCM. There’s an opportunity to build upon this and reverse disease. The research out of Penn reinforces the value of immunotherapy beyond cancer and establishes the use of mRNA to reprogram T-cells particularly for chronic disease. On the latter, transient CAR-T cells are required for cardiovascular disease among others to limit toxicities and allow for safe repeat dosing.
The most generalizable part of this work is ID’ing pathogenic fibroblasts. The 2019 paper was centered on this. Once they figured out they could clear activated fibroblasts, the group analyzed RNA-seq data from 238 left ventricular tissue samples. A few genes were found to be upregulated when a patient had hypertrophic cardiomyopathy (HCM) or dilated cardiomyopathy (DCM). Fibroblast activation protein (FAP) had the greatest fold change in disease samples compared to controls. Combined with the observation that FAP is essential for embryonic development and is expressed at lower levels in adulthood, made it the best candidate to ID pathogenic/activate fibroblasts versus quiescent ones. The harder work is then formulating a candidate that can specifically deliver a cargo to a T-cell and measure clearance of activated fibroblasts.
This paper touches upon a few broader themes that are important for other companies and unveil new threads to pull on in biotech:
Curative medicines for common diseases
Extending precision medicine plus immunotherapies beyond cancer
Prerequisites for early-stage intervention and drug development
Cell and gene therapies have offered long-term cures for some patients but at a pretty high cost (>$500K and up to $2M for a treatment). To extend these technologies to autoimmunity & cardiovascular disease, manufacturing COGS need to come down substantially. Like an order of magnitude. This might end up happening by the next decade but not anytime soon given the technical difficulties to scale and reduce variability of CGT biomanufacturing runs. As a result, curative drugs will probably only be feasible for patient subsets that are numbered in the 10Ks, not millions. Still impactful but not at scale. This is where bispecifics and other novel biological formats can shine. Another consideration is long-term toxicities. This is a big reason why gene therapies are in a mini-dark age - their long-term effects are still being determined and influencing clinical trial progress. In short, curative medicines for large indications might need to be transient and redosable instead of one-and-done to sidestep this concern. But what should the price of a “cure” be if it might have to be dosed again? Nobody really knows and that's why medicines like Zolgensma are the canary in the coal mine to figure this all out for others to build on top of.
A common theme in biotech is to apply the success of immunotherapy to other diseases especially in neurodegeneration and autoimmunity. Companies like Alector emerged to bring this approach to diseases like Alzheimer’s. While others like Cabaletta and Sonoma for autoimmunity. Fibrosis fits particularly well here given that fibroblasts behave almost like cancer cells in many diseases. For example, in idiopathic pulmonary fibrosis (IPF), they overgrow in the lung, disrupt lung structures, and ultimately block airways. Fibroblasts can do this by immune system evasion. Similar to a cancer cell. And for fibrosis, finding a CTLA-4 or PD-L1 equivalent would lead to a golden age for heart disease, kidney, and more.
Lastly, success of a cell therapy for fibrosis mainly depends on the stage of the disease. The 2022 paper uses injured models that may not represent a specific cohort of heart failure. In general, fibrosis is a scarring process highlighted by the accumulation of fibroblasts & extracellular matrix (ECM) outgrowth. In short, you might be able to clear out the fibroblasts using a T-cell but the ECM deposits will remain. To be able to cure something like IPF, early-stage diagnostics are needed to catch patients before there is too much scarring. On this theme, 2 things that are obvious is that: (1) Liquid biopsies will enable cancer vaccines and (2) Similarly, better diagnostics will enable improved fibrosis medicines, which is not too hard to know given this arc played out in cancer over the last 2 decades.
Specifically for heart disease, fibroblasts are poorly characterized even if they are one of the most well-studied cell types in general. It’s because cardiac fibroblasts are a pleiotropic cell. The heterogeneity of cardiac fibroblasts hasn’t been fully captured yet, nevertheless linking them to disease phenotypes. Studying the origins of this cell type, coming from both endothelial cells and bone marrow progenitors, will help answer a few key questions:
What is the number of fibroblasts in the heart?
What are the subtypes and their role in development? Role in function and repair?
What makes cardiac fibroblasts only function in the heart and not other tissues? Response to contraction/pressure?
These questions might seem straightforward. But isolating fibroblasts and their progenitors has been challenging. Target ID for unique cell surface markers will not only be valuable for drug development but also to study fibroblast development.
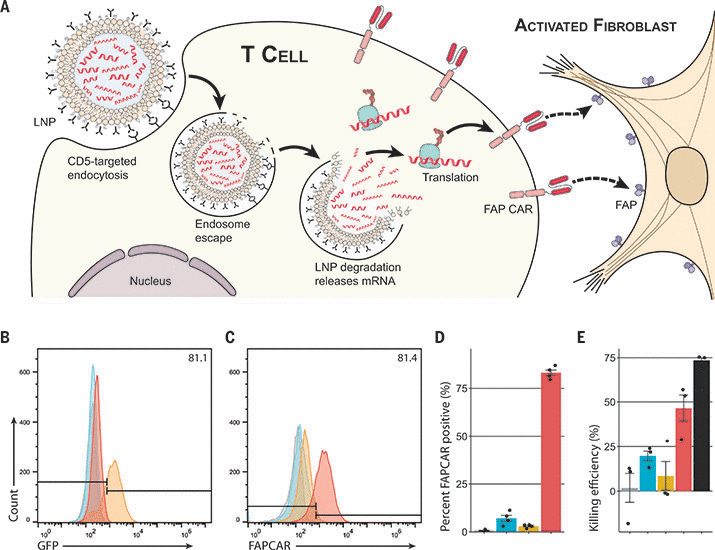
For the 2022 paper, after target identification, the key steps are LNP formulation, T-cell delivery, and finally restoring cardiac function. LNPs = lipid nanoparticles and probably represent one of the most exciting IP land grabs ongoing in biotech. The group packaged mRNA encoding a CAR for FAP, stabilized by pseudouridine incorporation, into an LNP that was decorated with a CD5 antibody. CD5 is a T-cell marker and allows for more specific LNP delivery. The key experiment here is delivering this cargo to murine T-cells in vitro (48 hour incubation). Around 83% of T-cells expressed the FAP-CAR construct. LNPs decorated with an IgG antibody control only successfully delivered the mRNA to ~7% of cells. This data was then validated in human T-cells with 89%-93% delivery success rates. The next step is validating T-cell reprogramming in vivo. The paper did a variety of experiments, from using luciferase mRNA to Cre/recombinase systems, to measure delivery to specific immune cell subtypes.
The last part is to assess if the LNP/CAR treatment can improve cardiac function in a mouse model. Using a AngII/PE mouse model for heart failure, 10 mg of the LNP was injected through IV, and after 2 weeks, the heart was analyzed with an echocardiogram. Left ventricular diastolic function returned to levels seen in the uninjured model: ~20 E/e′. Corresponding to this, CD3+ T-cells were over-accumulated around FAP-positive fibroblasts and over 50% of the T-cells expressed the FAP-CAR construct. On a macro level, the heart weight to bodyweight ratio returned to normal. With an n of 12, these studies still need to be replicated under a variety of conditions and across more models. However, these results establish 2 important things: an ability to produce functional CAR-T cells in vivo and restore heart function with a cell therapy. With the caveat: “in mice.”
The use of mRNA can allow for transient reprogramming of T-cells, limiting toxicities, and improving dosing. This is the important breakthrough to start bringing drugs like CAR-T to large diseases. With this technological approach, other tools from early-stage diagnostics to immunotherapies can be used to reverse chronic diseases. It’s not clear what beyond cancer will benefit from this triumvirate. It could be fibrosis but more of these experiments have to be reproduced and then translated. Neurodegeneration is the largest opportunity but the hardest. And autoimmunity has a shot but hit a clinical roadblock recently. All-in-all, the power to engineer the human immune system is unlocking more creative approaches to treat then cure disease.